
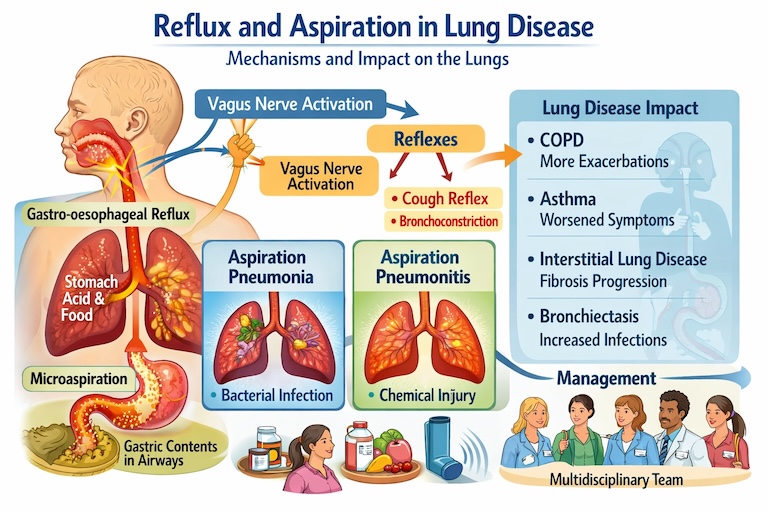
Reflux and aspiration lung disease can drive cough, wheeze, infections and longer-term airway and parenchymal damage, even when heartburn is absent. When gastric or oropharyngeal contents reach the larynx, trachea or distal airways, they can trigger chemical injury, introduce bacteria, alter the airway microbiome, and sustain inflammation that worsens pre-existing lung conditions.
How reflux can affect the lungs: the main mechanisms
Gastro-oesophageal reflux becomes clinically important for the lungs when it contributes to aspiration or to reflex airway responses. These are the key pathways.
1) Direct microaspiration of gastric contents
Small-volume “silent” aspiration can occur during sleep or after meals, particularly with supine positioning, impaired swallow, sedating medicines, neurological disease, frailty, or poor laryngeal protection. Refluxate may contain acid, pepsin, bile salts and food particles. Even tiny, repeated exposures can irritate the epithelium, disrupt mucociliary clearance, and prime the airway for infection and remodelling.
Why this matters clinically: repeated microaspiration can look like “difficult asthma”, “recurrent infective exacerbations”, or an unexplained progression of bronchiectasis or fibrotic ILD. Patients may not report classic reflux symptoms.
2) Chemical injury and sterile inflammation
Acid and bile salts can injure airway and alveolar tissue. The lungs respond with neutrophilic inflammation, increased epithelial permeability, surfactant dysfunction, and bronchial hyperreactivity. This mechanism is central in aspiration pneumonitis (see below), but it can also operate at a low level in chronic microaspiration.
3) Bacterial seeding and aspiration of oropharyngeal secretions
Not all aspiration starts in the stomach. Aspiration of bacteria-rich saliva and oropharyngeal secretions is a major driver of aspiration pneumonia in people with swallowing impairment. The bacterial load rises with poor dentition, dry mouth, and inadequate oral care.
4) Oesophago–bronchial reflexes (vagal reflex bronchoconstriction)
Reflux into the distal oesophagus can trigger vagally mediated cough and bronchoconstriction without aspiration. This can worsen wheeze, cough, nocturnal symptoms, and perceived breathlessness. It also complicates interpretation: treating reflux may reduce symptoms even when aspiration tests are negative, and vice versa.
5) Mechanical interaction with lung disease
Hyperinflation in COPD can flatten the diaphragm and change pressure gradients across the lower oesophageal sphincter. Chronic cough and frequent use of bronchodilators may also affect reflux dynamics. In advanced lung disease, increased work of breathing and posture changes can further promote reflux and aspiration risk.
Aspiration syndromes: pneumonia, pneumonitis, and chronic microaspiration lung disease
Aspiration pneumonia
Aspiration pneumonia is infection that follows aspiration of colonised secretions (often oropharyngeal). It tends to occur in older adults, people with dysphagia, neurological disease, reduced consciousness, or poor oral hygiene. Clinically, you see fever, purulent sputum, focal chest signs and radiographic consolidation (often dependent segments). The key point is infection: antibiotics are usually required, alongside prevention strategies (swallow management, oral care, positioning).
Aspiration pneumonitis
Aspiration pneumonitis is a chemical injury from a larger-volume aspiration event, typically sterile gastric contents. It can cause sudden hypoxaemia, bronchospasm and diffuse infiltrates. Early features may mimic infection, but inflammation drives the initial injury. Patients can improve with supportive care alone, although secondary infection can develop later. Over-treating every aspiration pneumonitis with prolonged antibiotics exposes patients to harm without clear benefit, so clinical judgement and reassessment are essential.
Chronic microaspiration-related lung disease
Chronic microaspiration sits between these extremes. Repeated, small insults can lead to:
- Chronic cough and throat clearing
- Laryngeal irritation and hoarseness
- Poorly controlled asthma-like symptoms
- Recurrent “infective” exacerbations with variable bacterial yield
- Airway remodelling (bronchial wall thickening, small airway disease)
- Bronchiectasis progression in susceptible patients
- Potential contribution to fibrotic ILD progression in some phenotypes (association strongest in IPF literature, but causality remains debated)
Because microaspiration is often silent, diagnosis relies on pattern recognition plus targeted testing rather than symptoms alone.
Impact on specific lung diseases: prevalence, progression and exacerbations
COPD
How common is reflux in COPD? Estimates vary by definition and population, but reflux is consistently reported as a frequent comorbidity. More importantly, multiple studies link GERD with exacerbation risk.
Clinical implication: in frequent exacerbators, reflux/aspiration assessment can become as important as checking inhaler technique or eosinophils.
What does it do to outcomes? A meta-analysis of observational studies found GERD associated with a markedly increased risk of COPD exacerbation (reported odds ratio 5.37) and a higher exacerbation frequency (weighted mean difference 0.48 exacerbations). This does not prove causation, but it supports routine consideration of reflux/aspiration when someone has frequent exacerbations despite guideline-based inhaled therapy.
Asthma
How common is reflux in asthma? Reflux appears common, and it can present as nocturnal cough, throat symptoms, or “non-allergic triggers”. However, symptom-based diagnosis overestimates true reflux, while silent reflux may be missed.
Reflux can increase symptoms and exacerbate asthma via microaspiration and vagal reflexes. An ATS commentary highlights links between GERD and increased asthma exacerbations and worse asthma-related quality of life.
Does treating reflux improve asthma control? The evidence is mixed. Proton pump inhibitor (PPI) therapy shows only small average improvements in lung function measures in adults, and benefits concentrate in patients with clear reflux symptoms or documented reflux. If asthma remains poorly controlled, the clinician should avoid assuming reflux is “the” cause; it may be one contributor among many (adherence, allergens, obesity, inducible laryngeal obstruction, eosinophilic inflammation).
Interstitial lung disease, especially IPF
Reflux is reported as highly prevalent in IPF cohorts, often without classic symptoms. A landmark study reported abnormal acid gastro-oesophageal reflux in 87% of IPF patients. More recent work in broader ILD populations continues to report a high prevalence of abnormal reflux while emphasising uncertainty about direction of causality (does reflux drive fibrosis, or does ILD promote reflux mechanics?).
Biologic plausibility is strong (microaspiration as a repetitive epithelial injury), but interventional evidence is less definitive. Some earlier observational signals suggested anti-reflux therapy might relate to slower progression in IPF, yet later analyses and trial-era data have been more cautious.
Practically, clinicians should treat symptomatic reflux and address aspiration risk, but they should avoid overselling anti-reflux therapy as a proven anti-fibrotic strategy.
Bronchiectasis
How common is reflux in bronchiectasis? Reviews describe a wide prevalence range, roughly 26% to 75%, including clinically silent reflux.
Co-existing reflux correlates with worse bronchiectasis severity, more symptoms and exacerbations, more hospitalisations, and poorer quality of life in several studies.
The likely mechanisms include microaspiration increasing airway inflammation, impairing clearance, and encouraging chronic infection. In patients with bronchiectasis who repeatedly grow the same organisms (particularly enteric gram-negative bacteria), reflux/aspiration can act as a “hidden feeder” of airway bacterial burden.
Management: prevention and treatment with a multidisciplinary team
Because reflux and aspiration cross aerodigestive boundaries, the best care is multidisciplinary. The MDT often includes a pulmonologist, gastroenterologist, ENT, speech and language therapist (SLT), specialist respiratory physiotherapist, dietitian, nursing team, and (when needed) neurology and palliative care.
The pulmonologist’s role (often the coordinator)
Pulmonologists commonly pull the story together because patients present with cough, wheeze, infections or breathlessness, and exacerbations of chronic respiratory disease. Key responsibilities include:
- Phenotyping the lung disease (asthma endotype, COPD exacerbator phenotype, bronchiectasis severity, ILD pattern)
- Identifying aspiration clues: nocturnal cough, wet voice after drinks, recurrent right lower lobe changes, frequent “infective” flares with modest CRP, or persistent radiographic dependent changes
- Requesting and interpreting lung-focused tests: CT patterns (dependent tree-in-bud, centrilobular nodules, bronchiectasis distribution), sputum microbiology, spirometry, FeNO/eosinophils, and exacerbation diaries
- Triggering the MDT: early SLT referral for suspected dysphagia, physiotherapy for airway clearance, gastroenterology for reflux evaluation, and dietetics for safe nutrition plans
Practical assessment pathway
- Risk and symptom screen: dysphagia, choking, wet voice, dentition, sedatives/opioids, neurological disease, supine sleep, late meals, alcohol.
- Swallow evaluation: bedside SLT assessment, and when indicated videofluoroscopy (VFS)
- Reflux testing (selectively): 24-hour pH impedance (captures non-acid reflux), manometry.
- Airway sampling and imaging: sputum culture, CT chest, and bronchoscopy.
Prevention strategies that often matter more than drugs
- Positioning: head-of-bed elevation, avoid lying flat after meals
- Oral hygiene: reduces bacterial load and aspiration pneumonia risk
- Optimising swallow safety: texture modification only when clearly helpful; supervised feeding when needed; pacing and fatigue management
- Medication review: reduce sedatives, anticholinergics, and drugs that impair swallow where feasible
- Airway clearance techniques (ACTs): particularly in bronchiectasis and chronic aspiration with ineffective cough
- Nutrition planning: balancing aspiration risk with malnutrition risk, sometimes requiring enteral feeding decisions
Treating reflux: what to use and when
- Lifestyle measures first where possible (meal timing, weight management, reducing triggers).
- PPIs: best for acid-mediated symptoms and oesophagitis; less reliable for non-acid reflux and aspiration risk. Consider time-limited trials with clear goals (symptom reduction, exacerbation reduction), and stop if no benefit.
- Prokinetics: sometimes considered, but adverse effects limit long-term use.
- Anti-reflux surgery (e.g., fundoplication): may help selected patients with proven reflux and respiratory complications, but patient selection is crucial and evidence quality varies by population.
Frequently asked questions
1) Can reflux cause lung scarring?
It may contribute in some patients through repetitive microaspiration and epithelial injury, especially discussed in IPF, but causality is not fully proven and treatment of reflux is not a guaranteed way to slow fibrosis.
2) How can I tell aspiration pneumonitis from aspiration pneumonia?
The two can be difficult to distinguish. Pneumonitis often follows a clear aspiration event with rapid breathlessness and inflammation that can mimic infection; pneumonia more often develops with fever, purulent sputum and evolving consolidation. Clinicians often reassess over 24–48 hours to avoid unnecessary prolonged antibiotics.
3) Does a PPI stop aspiration?
PPIs reduce acidity, not the physical act of refluxing or aspirating. Non-acid reflux can still reach the airway, so symptoms or exacerbations may persist despite acid suppression.
4) Why do I have chest symptoms without heartburn?
Reflux can be “silent”, and aspiration can occur at night. Some people mainly experience cough, throat clearing, hoarseness or wheeze rather than classic heartburn.
5) Who should be involved in care?
Often a pulmonologist leads, supported by SLT (swallow), respiratory physiotherapy (airway clearance), gastroenterology (reflux testing/treatment), dietetics (safe nutrition), and sometimes ENT and neurology depending on the cause.
GET IN TOUCH
Schedule a Visit with Dr Ricardo Jose
Disclaimer: The information provided in this article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your healthcare provider with any questions you may have regarding a medical condition or treatment