
The prognosis of bronchiectasis has changed significantly over the past two decades. Structured scoring systems now allow clinicians to estimate mortality risk, hospital admissions and future exacerbations with reasonable accuracy. These tools are based on large international patient cohorts and long-term follow-up studies.
However, they estimate risk, not certainty. They help doctors identify patterns seen across thousands of patients and apply them to the individual sitting in clinic.
Below, the evidence behind the most widely used prognostic tools is discussed.
The FACED Score: Development and Validation
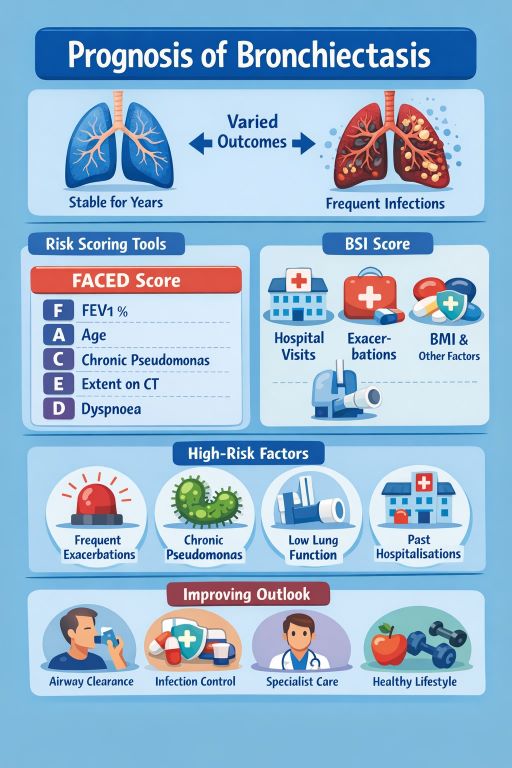
The FACED score was developed in Spain in 2014 using a large multicentre cohort of patients with stable disease. Researchers analysed clinical variables and identified five independent predictors of mortality:
- FEV1 (lung function)
- Age
- Chronic colonisation with Pseudomonas aeruginosa
- Radiological extent
- Dyspnoea severity
They followed patients for five years and examined survival outcomes.
What the Study Found
The original validation study showed:
- Clear separation between mild, moderate and severe groups.
- Five-year survival exceeded 90% in mild disease.
- Severe FACED scores were associated with markedly reduced survival.
- The model demonstrated strong statistical discrimination (high area under the curve values in ROC analysis).
Importantly, FACED performed consistently when tested in external international cohorts, including Latin American and European populations. This strengthened confidence in its reliability.
Strengths of FACED
- Simple and quick to calculate.
- Good predictor of 5-year mortality.
- Easy to apply in routine outpatient clinics.
Limitation Identified in Studies
Researchers later observed that FACED did not adequately predict future exacerbations or hospital admissions. Patients with relatively low mortality risk could still experience frequent flare-ups.
E-FACED: Adding Exacerbation Risk
E-FACED expanded the original score by including exacerbation frequency in the preceding year.
When tested in subsequent validation studies:
- E-FACED improved prediction of hospital admissions.
- It retained strong mortality prediction accuracy.
- It better identified patients at risk of disease progression.
Studies comparing FACED and E-FACED demonstrated statistically significant improvement in predicting short-term clinical deterioration.
For clinicians, this made E-FACED more useful in everyday management decisions.
Bronchiectasis Severity Index (BSI): A Broader Approach
The Bronchiectasis Severity Index was developed in the UK and validated internationally. Researchers followed patients for up to four years and examined:
- Mortality
- Hospital admissions
- Exacerbations
- Quality of life decline
Unlike FACED, BSI includes:
- BMI
- Prior hospitalisation history
- Prior exacerbation frequency
- Microbiological profile beyond Pseudomonas
- Radiological severity
What the BSI Studies Found
The original BSI study showed:
- Clear stratification of low-, moderate- and high-risk groups.
- High-risk patients had significantly greater hospital admissions.
- Mortality risk rose sharply in the high-risk group.
- Strong predictive power across multiple outcomes.
When directly compared to FACED in validation studies:
- BSI predicted hospital admissions more accurately.
- BSI better predicted future exacerbations.
- FACED remained slightly more streamlined for mortality prediction.
In statistical comparisons, BSI generally showed higher discriminatory power for healthcare utilisation outcomes.
FACED vs BSI: What the Evidence Says
Head-to-head comparative studies revealed:
- Both tools predict mortality reliably.
- BSI is superior for predicting exacerbations and admissions.
- FACED is easier and faster to calculate.
In clinical practice, many respiratory specialists favour BSI for comprehensive assessment and E-FACED when a simplified mortality-focused estimate is sufficient.
Neither model achieves perfect individual accuracy. Predictive models typically achieve “good” but not “excellent” discrimination. This means they correctly classify most, but not all patients into appropriate risk groups.
Accuracy of Prognostic Models: What Does “Accurate” Mean?
In medical statistics, accuracy is measured using:
- Area under the ROC curve (AUC)
- Calibration testing
- External validation
Most bronchiectasis scoring tools achieve AUC values between 0.70 and 0.85 for mortality prediction. In clinical research terms, this is considered moderate to good predictive performance.
This means:
- They reliably separate high-risk from low-risk groups.
- They are less precise in predicting exact survival timelines for individuals.
No current model can predict exactly how long a specific person will live. They estimate probability, not certainty.
Additional Prognostic Factors Identified in Research
Large registry studies and long-term observational data have identified consistent independent risk factors:
Chronic Pseudomonas aeruginosa Infection
Repeated studies show that persistent colonisation increases:
- Mortality risk
- Exacerbation frequency
- Hospital admission rates
It remains one of the strongest negative prognostic markers.
Frequent Exacerbations
Patients experiencing three or more exacerbations per year show:
- Accelerated lung function decline
- Increased healthcare use
- Higher mortality risk
Reduced Lung Function
Lower baseline FEV1 consistently correlates with worse outcomes across all models.
Low BMI
Underweight patients demonstrate higher mortality risk, likely due to frailty and systemic inflammation.
Prior Hospitalisation
Previous admissions predict future admissions. This pattern is strong and reproducible across international cohorts.
What About Radiological Severity?
High-resolution CT findings correlate with outcome, but not perfectly.
Studies show:
- Greater lobar involvement increases risk.
- Cystic bronchiectasis is associated with more severe disease.
- Radiology alone cannot predict prognosis without clinical context.
Real-World Reliability
When applied in routine clinical practice:
- Scores perform similarly to research settings.
- They help identify patients needing aggressive management.
- They guide decisions about referral to specialist centres.
Importantly, prognosis may change over time. Reassessment improves accuracy.
Emerging Prognostic Tools
Recent research explores:
- Blood inflammatory markers (CRP, neutrophil counts)
- Sputum microbiome profiling
- Biomarker panels
- Machine learning risk models
How Doctors Use Prognosis in Shared Decision-Making
Doctors do not use these scores to give rigid predictions. Instead, they use them to:
- Explain relative risk clearly.
- Identify modifiable factors.
- Intensify treatment for high-risk individuals.
- Provide reassurance to low-risk patients.
- Plan follow-up frequency.
For patients, the key message is that a high-risk score signals the need for closer monitoring and more proactive treatment. It does not indicate immediate deterioration.
Key Points
- The prognosis of bronchiectasis can be estimated using validated scoring systems.
- FACED predicts mortality effectively.
- E-FACED improves prediction of exacerbations.
- BSI offers the most comprehensive risk assessment.
- Accuracy is moderate to good, but not absolute.
- Regular reassessment improves reliability.
- Early and consistent management can modify risk.
- A doctor that knows you and your condition well can over individual sight.
Frequently Asked Questions
1. Are bronchiectasis prognostic scores reliable?
Yes. They are validated across multiple international studies and reliably identify high- and low-risk groups.
2. Which score is most commonly used?
BSI is widely used for comprehensive assessment. FACED and E-FACED are also common.
3. Can a high score improve over time?
Yes. Effective treatment and reduced exacerbations can lower risk classification.
4. Do these scores predict exact life expectancy?
No. They estimate probability of risk, not precise survival timelines.
5. Should all patients have a severity score calculated?
Most specialist clinics use them, especially in moderate to severe disease.
GET IN TOUCH
Schedule a Visit with Dr Ricardo Jose
Disclaimer: The information provided in this article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your healthcare provider with any questions you may have regarding a medical condition or treatment