Bronchiectasis is a lung disease characterised by the permanent widening of the bronchial tubes, causing them to lose their normal shape and ability to clear mucus.
Clinically it is associated with cough, production of phlegm (mucus) and recurrent chest infections.
Bronchiectasis is a complex disease with a multifactorial pathogenesis that involves damage to the airways and an ongoing cycle of infection and inflammation.
People with bronchiectasis may experience a range of symptoms that affect their daily life and quality of life. Common symptoms include:
Contact Dr Ricardo José today to arrange a specialist assessment and personalised care.
The following are some of the key steps in the development and progression of bronchiectasis:
A detailed history and examination, as well as targeted investigations can identify the cause of bronchiectasis in many cases. However, a proportion will be labelled “idiopathic” where the cause is unknown.
A mutation in the cystic fibrosis transmembrane regulator gene (CFTR) on chromosome 7 results in thick mucus that blocks ducts in various organs (e.g. lungs, pancreas, liver, intestines, cervix, vas deferens). To get the disease a person needs to acquire an abnormal gene from each parent.
The diagnosis is made from the clinical history, a chloride sweat test and genetic testing.
Treatment differs from that in non-CF bronchiectasis particularly with the novel medication (e.g. Kaftrio) for patients with specific gene mutations.
Primary Ciliary Dyskinesia (PCD) is also known as immotile cilia syndrome. It is an inherited condition associated with ciliary abnormalities. Cilia are hair-like structures attached to cells of the lining of the upper and lower respiratory tract, the eustachian tube, the cochlear in the ears and the male vas-deferens (a duct that transports sperm form the epididymus to the ejaculatory canal). When these cell don’t function normally they results in abnormal clearance of mucus in the airways and chest infections, sinus and ear infections, loss of hearing and infertility. During development of the fetus cilia are also responsible for the movement of developing organs to their correct position and half of people affected by PCD can have dextrocardia (heart on the right side of the chest) or situs inversus where all the organs are on opposite sides.
The inability to clear mucus and recurrent chest infections results in bronchiectasis.
Parts of the immune system (immune cells or antibodies) are missing or not working properly mostly due to errors in the genes. The primary immunodeficiency disorders (PID) consist of over 300 conditions with a wide spectrum of disease severity. They are usually identified in childhood but some less severe conditions are only diagnosed later in life.
The impaired immune function predispose to recurrent and severe infections that often taken longer to improve on antibiotic therapy. Infections may be due to opportunistic pathogens that are harder to diagnose.
Once there is suspicion of a PID the diagnosis is usually by specialist laboratory tests carried out by an immunologist
Alpha-1 anti-trypsin (A1AT) is a protein that neutralises various proteases (e.g. neutrophil elastase) and protects organs such as the lungs from damaged cause by these proteases. A1AT deficiency is caused by a genetic mutation in the SERPINA 1 gene resulting in low levels of A1AT. Low levels of A1AT can’t protect the lungs from damage caused by inflammation following exposure to smoke or dust, or chest infections, resulting in tissue damage. People with A1AT are more likely to develop COPD at a younger age and can develop bronchiectasis. It is very important that people with A1AT don’t smoke. Also, screening of close relatives should be undertaken to establish a diagnosis and counsel on preventing lung disease.
The immune system can be affected by disease, medication and toxins. The impaired immune system results in recurrent and severe infections that take longer to improve on antibiotics. Infections may be due to opportunistic pathogens that are harder to diagnose.
Common diseases causing secondary immunodeficiency (SID):
Common treatments causing SID:
Infections of the lungs are probably the most common cause of bronchiectasis. These may be severe infections such as pneumonia and tuberculosis, or other childhood infections that may affect the chest such measles and Whooping cough. Often by the time bronchiectasis becomes a problem in adulthood the occurrence of childhood infections is not recalled. Importantly, aspiration pneumonia is also an important cause of bronchiectasis and is often seen in patients with head and neck cancer or post-stroke.
Allergic bronchopulmonary aspergillosis (APBA) is caused by an allergic immune reaction in the airways to the mould of the Aspergillus species. A similar condition when the allergy is due to other fungi and is termed allergic bronchopulmonary mycosis (ABPM). It usually occurs in patients with asthma and causes symptoms of shortness of breath, wheeze, cough (including coughing blood), mucus production and intermittent fevers.
The diagnosis is made clinically with the support of investigations confirming sensitisation to the fungus. The pattern of flitting consolidation and bronchoceles as well as obstructive lung function tests also support the diagnosis.
Treatment involves targeting the allergic inflammation in the airways with inhaled corticosteroids, oral corticosteroids (e.g. prednisolone) and anti-fungal medications (e.g. itraconazole, voriconazole and posaconazole)
More commonly seen in children, the obstruction of an airway by a foreign object can result in distal bronchiectasis and recurrent infections. A history of aspiration (e.g. during dental treatment) is important in considering the diagnosis that may be diagnosed on radiological imaging of the chest or at bronchoscopy.
Obstruction of the airway by a tumour can also result in distal bronchiectasis.
Connective tissue disorders are those where the tissue (e.g. tendons, ligaments, cartilage, skin, eyes) containing collagen and elastin that connects different parts of the body are inflamed.
They include:
Investigations are carried out to determine the presence of specific auto-antibodies in blood to establish the presence of a CTD.
CTD is associated with bronchiectasis with the presence of bronchiectasis sometimes predating the presentation of CTD features (painful and swollen joints, rashes, etc.)
Ulcerative colitis is an inflammatory disorder of the colon that results in symptoms of loose stools, abdominal pain and bloody bowel movements. It can also cause fevers, weight loss and fatigue and be associated with joint pain. The diagnosis is made by a gastroenterologist who will do a colonsocopy and take biopsies of the lining of the colon. A test of the faeces (fecal calprotectin) if low makes the disease unlikely.
Although the mechanism of how it affects the lungs isn’t known, bronchiectasis is associated with ulcerative colitis.
Diagnosing bronchiectasis usually involves several tests to confirm the condition, identify infections, and look for underlying causes. These investigations help guide treatment and long-term management.
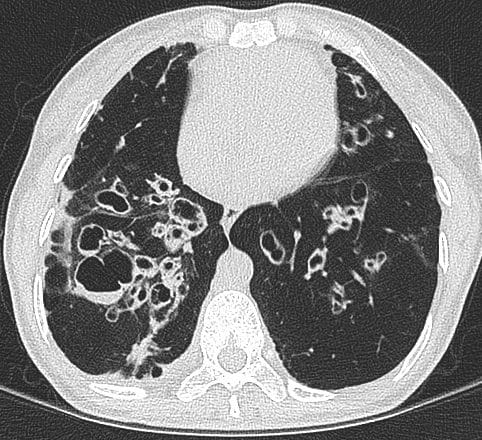
A high-resolution CT scan of the chest is the most important test for diagnosing bronchiectasis. It allows doctors to see widened or damaged airways in the lungs. A chest X-ray may also be performed, but CT scanning provides much more detailed images.
Sputum samples are analysed to identify infections in the lungs. These cultures look for bacteria, mycobacteria such as tuberculosis, and fungi. Identifying the specific organism helps guide antibiotic treatment.
Breathing tests measure how well the lungs are working and how easily air moves in and out. These tests can also identify co-existing conditions such as asthma or airflow obstruction.
Blood tests may be used to look for inflammation and to investigate possible causes of bronchiectasis. These may include tests of immune function or genetic tests where appropriate.
This may include a sweat chloride test and genetic testing to look for cystic fibrosis, particularly in younger patients or when symptoms suggest this condition.
This condition affects the movement of microscopic hairs (cilia) that clear mucus from the airways. Tests may include measurement of nasal nitric oxide, specialised nasal brush samples, and genetic testing.
Management of bronchiectasis focuses on controlling symptoms, reducing infections, and preventing further lung damage. Treatment is tailored to each patient because disease severity, underlying causes, and infection patterns vary between individuals. Dr Ricardo José has extensive experience in diagnosing and managing bronchiectasis and provides a comprehensive assessment to develop a personalised treatment plan.
The first step in treatment is confirming the diagnosis and identifying the cause of bronchiectasis. Dr Ricardo José carefully reviews previous imaging, including CT scans of the chest, to confirm the diagnosis and assess the severity of airway damage. He also reviews sputum culture results to identify infections and performs lung function tests to evaluate how well the lungs are working.
Dr José frequently provides second opinions for patients with respiratory symptoms and diagnoses. In some cases, patients previously diagnosed with asthma or COPD are found to have underlying bronchiectasis. In others, patients who have been labelled as having bronchiectasis may actually have a different respiratory condition. Careful reassessment helps ensure the correct diagnosis and the most appropriate treatment plan.
He may also request blood tests or specialised investigations to identify underlying conditions that can contribute to bronchiectasis.
By confirming the diagnosis and identifying both the cause and severity of the disease, Dr José can develop the most appropriate and personalised treatment strategy.
Dr Ricardo José provides access to the full range of treatments used to manage bronchiectasis. He develops personalised treatment plans based on each patient’s symptoms, infection history, and the severity of their condition. Management may include airway clearance therapy, targeted antibiotics, inhaled medications, and strategies to prevent recurrent infections.
Dr José works closely with highly experienced respiratory physiotherapists who specialise in airway clearance techniques for bronchiectasis. This collaborative approach helps patients learn effective methods to clear mucus and reduce the risk of infections.
For patients who require more intensive treatment, Dr José has admitting rights at the Royal Brompton Hospital and The London Clinic, allowing access to inpatient care when intravenous antibiotics are needed. Patients may also receive intravenous antibiotic treatment through outpatient services, including the Royal Brompton Hospital day unit, or through home antibiotic therapy where appropriate.
In some cases, nebulised antibiotics may be recommended to help control chronic airway infections and reduce the frequency of flare-ups. This comprehensive approach ensures that patients have access to the full range of specialist treatments for bronchiectasis.
Airway clearance is the mainstay of bronchiectasis management and it is important to get the advise of a specialist respiratory physiotherapist.
This may involve the following techniques:
Sometimes adjuncts are needed to help expectorate the phlegm including the use of an Acapella or Aerobika flutter valves or a positive expiratory pressure (PEP) valve.
Medication can also be used to help alter the viscocity of the mucus and assist with clearance. Nebulised saline (NaCl) is often used with concentrations ranging from 0.9% (isotonic) to 7% (hypertonic) as well as other mucolytics such as carbocisteine.
The treatment of active chest infections and exacerbations of bronchiectasis is with antibiotics. In individuals with bronchiectasis these need to be tailored at the usual pathogens that are cultured in the sputum and for an appropriate duration (usually 10 – 14 days).
Prophylactic (preventative) antibiotics are usually prescribed when there is a history of frequent infections or exacerbations of bronchiectasis (3 or more in 12 months). depending on the individual case these may be recommended seasonally or all year round. Prophylactic antibiotics may be given orally or in some cases via the nebulised route.
Azithromycin is an antibiotic with immunomodulatory properties. In addition to its ability to stop bacteria from growing it is able to change the way the immune system functions or responds. It has been shown to reduce the frequency of bronchiectasis exacerbations in patients with Pseudmonas aeruginosa infections and to reduce phlegm volume.
It is recommended that patients with bronchiectasis receive the annual influenza (Flu) vaccination and the pneumococcal polysaccharide vaccine (PPV23) if they have low total pneumococcal or specific pneumococcal serotype antibody levels. Some times other vaccines are adminsitered as part of testing of the immune system function (e.g. tetanus vaccine).


Dr Ricardo José provides specialist assessment and personalised care for people with bronchiectasis across both the NHS and private sector. He runs several bronchiectasis-related clinics, including new patient clinic, follow-up bronchiectasis clinics (including fungal and mycobacterial lung disease, an immunodeficiency-related respiratory clinic and a primary ciliary dyskinesia clinic. He also looks after inpatients that need hospital care for bronchiectasis and complex respiratory infections. This breadth of clinical experience means he regularly sees patients with complex bronchiectasis, recurrent infections and underlying conditions that can contribute to ongoing respiratory symptoms.
During your consultation, Dr José will review your symptoms, medical history, infection pattern, lung function and scan results to build a treatment plan tailored to you. This may include identifying underlying causes, optimising airway clearance, managing infections, reviewing inhaled or antibiotic treatments, and supporting prevention strategies such as vaccination and flare-up planning.
Patients see Dr José for a thorough, evidence-based approach to bronchiectasis care, with a focus on improving day-to-day symptoms, reducing the risk of future chest infections and helping people feel more confident managing their condition. Whether you have recently been diagnosed or are experiencing frequent flare-ups despite treatment, Dr José can provide expert guidance and ongoing respiratory support.
Contact Dr Ricardo José today to arrange a specialist assessment and personalised care.
Bronchiectasis is a chronic lung condition where the airways (bronchi) become permanently widened, inflamed and scarred, leading to mucus build-up that’s hard to clear. This makes infections more frequent and breathing more difficult over time.
Common symptoms include a persistent cough that produces large amounts of mucus (sputum), recurrent chest infections, breathlessness, fatigue, wheezing, and sometimes coughing up blood. Symptoms vary in severity and often worsen during infections.
Diagnosis usually involves medical history, a physical exam, and imaging — especially a high-resolution CT scan — which shows widened airways, thickened airways and mucus plugging.
Bronchiectasis can develop after lung infections (like pneumonia), from conditions that affect immunity or lung health (like COPD or asthma), genetic disorders like cystic fibrosis, or sometimes with no identifiable cause. Risk increases with age and underlying lung problems.
There is no single “best” treatment for bronchiectasis. Management usually focuses on clearing mucus from the lungs, treating infections, and preventing flare-ups. Common treatments include airway clearance physiotherapy, antibiotics for infections, and sometimes inhaled medications or long-term antibiotics in people with frequent exacerbations. Treatment needs to be personalised to each person’s condition.
An exacerbation or flare-up is when symptoms suddenly worsen, usually due to infection. This may include increased coughing, more mucus, chest pain or shortness of breath. Early treatment, often with antibiotics and adjustments to airway clearance, can help resolve the flare-up and prevent further lung damage.
Life expectancy for someone with bronchiectasis can vary widely depending on the severity of the condition, the underlying cause, and how well it is managed. Many people with mild or well-controlled bronchiectasis can live a normal or near-normal lifespan. However, more severe disease, frequent infections, or complications affecting lung function may reduce life expectancy in some cases.
To learn more about how doctors assess outlook and disease severity, you can read the article on determining prognosis in bronchiectasis.
Dr Jose is a superlative physician. He was extremely thorough, took great care to listen to the complicated history of my mother’s illness, taking notes throughout and personally reviewing all prior testing. He explained both his thoughts on her illness and his recommendations clearly and went out of his way to organise next steps for us. He remained in contact throughout and communicated both with us and other medical professionals involved in her care. I am a doctor myself and highly recommend dr Jose to anyone who is looking for an experienced, knowledgeable and compassionate respiratory physician.
Dr Ricardo Jose was a very kind and caring doctor. He listened patiently to my health issues and offered an immediate suggestion for one of the issues. He also discussed plans for tests and treatments to alleviate and prevent future flare-ups/ infections. He is very experienced in my particular area of pulmonary issues and my consultation was a reassuring experience for me. Thank you so much
Speak with the team today to arrange an appointment with Dr Ricardo Jose.